Recognize Reed–Sternberg (“owl’s eye”) cells as the defining histopathologic hallmark of classic Hodgkin lymphoma.
Question - Biopsy finding
A 20-year-old man with no previous medical history has developed prominent lymphadenopathy in the left cervical chain. His lymph node is rubbery and firm. He also has developed malaise, poor appetite, weight loss, and fever associated with drenching night sweats. He assumed that the symptoms were related to the flu and initially did not pay attention to them, but he tells you that they have been ongoing for 3.5 weeks. In addition, he has developed mild cough. Upon admission, chest x-ray showed an enlarged mediastinum and computed tomography of the chest confirmed the presence of a mediastinal mass. Biopsy of the mass was obtained and a diagnosis of Hodgkin lymphoma was confirmed.
Which of the following abnormalities is likely to be seen in the biopsy sample?
Answer Options:
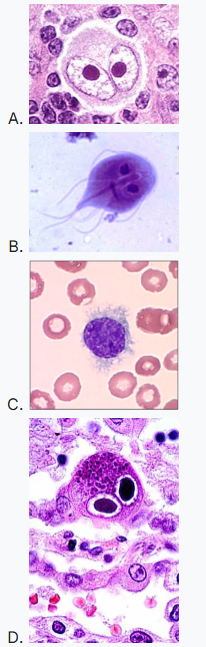
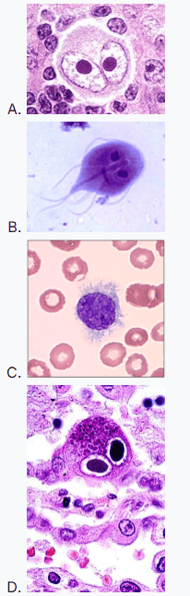
- Image A
- Image B
- Image C
- Image D
This is a boards-style “pattern recognition” item: a young adult with painless cervical lymphadenopathy, B symptoms (fever/night sweats/weight loss), and a mediastinal mass strongly suggests classic Hodgkin lymphoma (often nodular sclerosis subtype). The defining biopsy feature is the Reed–Sternberg cell—large atypical cells with bilobed/binucleate nuclei and prominent nucleoli (“owl’s eyes”) within a reactive inflammatory background.
This aligns with major consensus standards (e.g., WHO 2022; NCCN 2024/2025; ESMO 2020): Hodgkin lymphoma diagnosis is established by tissue biopsy demonstrating characteristic histology (Reed–Sternberg cells in classic HL) supported by immunophenotype (classically CD30+, often CD15+).
Why This Internal Medicine Question Is Often Missed
- “Owl’s eye” is tested in multiple diseases (Reed–Sternberg vs CMV inclusions vs Giardia), so learners anchor on the phrase rather than the clinical syndrome.
- Test-takers overvalue the mediastinal mass as a “thymoma/germ cell” clue and forget HL is a classic cause in young adults.
- Image-based distractors exploit confusion between blood smear parasites/leukemia cells and tissue pathology.
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| Image A |
Reed–Sternberg cell (classic Hodgkin lymphoma) |
Correct: fits HL biopsy finding (large binucleate/bilobed cell with prominent nucleoli). |
| Image B |
*Giardia lamblia* trophozoites (two nuclei) |
GI infection (malabsorption, watery diarrhea, bloating), not mediastinal mass + B symptoms + lymphadenopathy. |
| Image C |
Hairy cell leukemia smear (cytoplasmic projections) |
Typically middle-aged; findings include splenomegaly, pancytopenia, “dry tap,” not mediastinal mass HL syndrome. |
| Image D |
CMV “owl’s eye” intranuclear inclusions |
Seen in immunocompromised states (transplant, advanced HIV) with end-organ disease; not the classic HL biopsy hallmark. |
Internal Medicine High-Yield Pearl for Exam Prep
In a young adult with painless cervical LAD + B symptoms + mediastinal mass, the biopsy clue you must recognize is a Reed–Sternberg cell (classic HL).
Core Learning Objectives
- Identify the clinical syndrome suggestive of classic Hodgkin lymphoma in board-style vignettes.
- Recognize Reed–Sternberg cells as the defining histopathologic feature of classic Hodgkin lymphoma and distinguish from common “owl’s eye” mimics.
The Exam “Test Trick” at Play
The item weaponizes a shared visual descriptor (“owl’s eyes”) across unrelated entities (Giardia trophozoites and CMV inclusions) to test whether you prioritize *syndrome + tissue context* over a memorized phrase. Boards reward integrating age, distribution of lymphadenopathy, mediastinal involvement, and B symptoms with the correct pathology specimen.
Additional Internal Medicine Practice Questions and Remediation for Hodgkin Lymphoma Pathology
Internal Medicine Practice Question 1 — Young adult mediastinal mass
A 24-year-old woman has painless left supraclavicular lymphadenopathy, pruritus, and night sweats. CT shows an anterior mediastinal mass. Lymph node biopsy shows large atypical cells in an inflammatory background; tumor cells are CD30+ and usually CD15+. Most likely diagnosis?
- A. Primary mediastinal (thymic) large B-cell lymphoma
- B. Classic Hodgkin lymphoma, nodular sclerosis subtype
- C. Diffuse large B-cell lymphoma, NOS
- D. T-lymphoblastic lymphoma
- E. Metastatic seminoma
Internal Medicine Practice Question 2 — “Owl’s eye” distinction
A transplant recipient develops colitis and fever. Biopsy shows enlarged cells with prominent basophilic intranuclear inclusions surrounded by a halo. What is the finding?
- A. Reed–Sternberg cells
- B. Cytomegalovirus inclusions
- C. Giardia trophozoites
- D. Hairy cells
- E. Touton giant cells
Internal Medicine Practice Question 3 — HL vs NHL pattern
Which feature most strongly favors Hodgkin lymphoma over non-Hodgkin lymphoma on typical board vignettes?
- A. Extranodal mass in the stomach
- B. Generalized peripheral blood involvement
- C. Contiguous spread from one lymph node group to the next
- D. Burkitt “starry-sky” pattern
- E. Mature plasma cell proliferation in marrow
Internal Medicine Practice Question 4 — Giardia mimic
A 30-year-old hiker has greasy foul-smelling diarrhea, bloating, and weight loss after drinking from a stream. Stool O&P shows pear-shaped organisms with two nuclei. What is the organism?
- A. Cryptosporidium
- B. Entamoeba histolytica
- C. Giardia lamblia
- D. CMV
- E. Reed–Sternberg cell
Internal Medicine Practice Question 5 — Hairy cell leukemia clue
A 55-year-old man has fatigue and recurrent infections. Exam shows splenomegaly. CBC shows pancytopenia; peripheral smear shows lymphocytes with cytoplasmic projections. Best associated finding?
- A. Mediastinal mass
- B. Cervical “B symptoms” presentation
- C. Bone marrow fibrosis with a “dry tap”
- D. CD30 positivity of malignant cells
- E. EBV-positive Reed–Sternberg cells as defining feature
Mini Case Discussion Prompt
How would your leading diagnosis and expected biopsy finding change if the same patient had chronic watery diarrhea after camping (with “two-nuclei” organisms) rather than mediastinal mass and B symptoms?
Mini-FAQ
Q1: What single cell type defines classic Hodgkin lymphoma on boards?
A: Reed–Sternberg cells; ABIM-style questions expect recognition of binucleate/bilobed giant cells with prominent nucleoli (“owl’s eyes”) in a reactive background.
Q2: Why is a mediastinal mass such a strong clue in a young adult?
A: Nodular sclerosis classic Hodgkin lymphoma commonly presents with mediastinal involvement; board vignettes often pair this with cervical/supraclavicular LAD and B symptoms.
Q3: How do I avoid confusing RS cells with CMV “owl’s eye”?
A: Use context: CMV inclusions occur in immunocompromised patients and are intranuclear inclusions in infected cells; RS cells are neoplastic lymphoid cells in lymph node architecture.
Q4: Do guidelines require excisional biopsy for diagnosis?
A: Yes in principle—major consensus (e.g., NCCN 2024/2025; ESMO 2020) emphasizes adequate tissue (excisional/incisional preferred; core in select cases) to demonstrate characteristic histology and immunophenotype.
This question appears in Med-Challenger Internal Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!