The exam-relevant concept is that ventilator dyssynchrony in obstructive disease is best reduced by aligning ventilator triggering/support with true patient effort—NAVA does this most directly among the listed options.
Question - Ventilator mode
You intubate a 9-year-old with refractory asthma.
Which mode of ventilation will reduce dyssynchrony with its attendant risk of ventilator-induced lung injury?
Answer Options:
A. Neurally Adjusted Ventilatory Assist (NAVA)
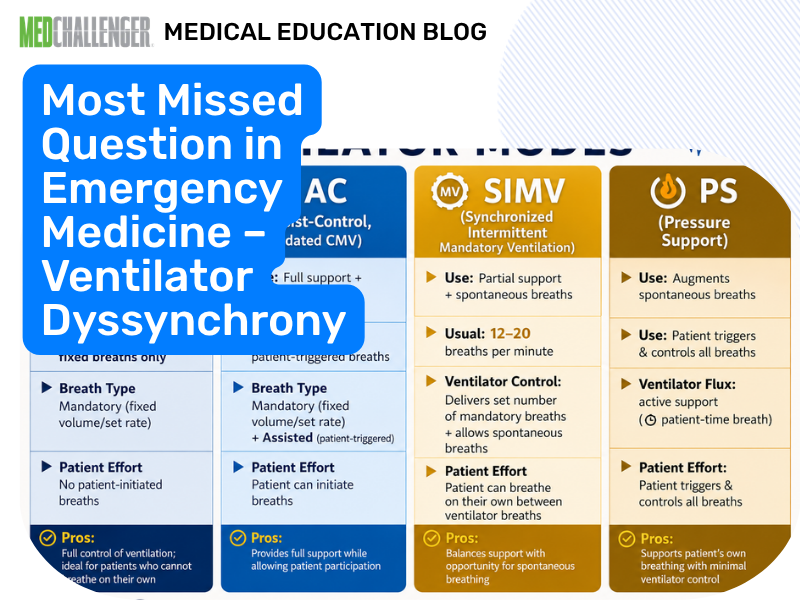
B. Synchronized intermittent mandatory ventilation (SIMV)
C. Assist-control ventilation
D. No positive end-expiratory pressure (PEEP)
Validated correction note: The keyed answer (A) is reasonable as the best choice among these options, but this question is frequently missed because NAVA is not a universal guideline-designated “standard” mode for intubated status asthmaticus; boards more commonly emphasize ventilator setting optimization (low rate, prolonged expiratory time), sedation, and managing auto-PEEP. Still, if the stem asks specifically for a mode that reduces dyssynchrony, NAVA is the most defensible answer choice.
NAVA senses the electrical activity of the diaphragm via an esophageal catheter and uses that signal to trigger and proportionally assist breaths. Because triggering is based on neural respiratory drive rather than airway pressure/flow changes, NAVA can substantially reduce trigger delay and asynchrony—particularly in obstructive physiology where auto-PEEP and dynamic hyperinflation interfere with conventional triggering.
This item illustrates a classic exam trap: learners correctly focus on asthma ventilation priorities (avoid air trapping, permissive hypercapnia, minimize minute ventilation), but the stem is narrowly asking about dyssynchrony reduction by ventilator mode. Among the listed choices, SIMV and assist-control are conventional modes that can still exhibit major asynchrony in auto-PEEP states unless carefully adjusted; “no PEEP” is not a ventilator mode and can worsen the work required to trigger breaths in the presence of intrinsic PEEP.
Why This Emergency Medicine Question Is Often Missed
- Many test-takers default to “assist-control” as a general ICU answer, but it does not inherently fix auto-PEEP–related triggering problems.
- NAVA is less familiar and not available on all ventilators, so learners under-select it despite the synchrony clue.
- Confusion between external PEEP strategy (to help overcome auto-PEEP) vs a ventilator mode.
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| NAVA |
Neural triggering proportional support to improve synchrony |
Correct for the asked concept: reduces dyssynchrony by matching ventilator assistance to diaphragmatic drive. |
| SIMV |
Partial mandatory breaths, spontaneous breaths between |
Does not inherently prevent dyssynchrony; spontaneous breaths still rely on flow/pressure triggering that can fail with auto-PEEP. |
| Assist-control |
Full support for triggered/mandatory breaths |
Conventional triggering can be ineffective with intrinsic PEEP; dyssynchrony can persist without careful adjustments/sedation. |
| No PEEP |
Misconception that zero PEEP avoids hyperinflation |
Not a “mode,” and zero external PEEP can increase trigger work when auto-PEEP is present (patient must generate more negative pressure to trigger). |
High-Yield Pearl for ABEM Exam Prep
In obstructive disease with auto-PEEP, dyssynchrony often stems from ineffective triggering—NAVA bypasses airway-pressure triggering by using diaphragmatic electrical activity.
Core Learning Objectives
- Distinguish which ventilator modes best reduce patient–ventilator dyssynchrony in obstructive physiology.
- Recognize how auto-PEEP contributes to ineffective triggering and why ventilator strategies that better detect patient effort reduce VILI risk.
The Exam Trick at Play
The stem tempts you to think about “asthma ventilator settings” broadly, but it asks specifically for a mode that reduces dyssynchrony. On many exams, uncommon but mechanistically precise options (like NAVA) are correct when the question highlights synchrony/triggering as the primary goal.
Additional Practice Questions & Remediation for Ventilator Dyssynchrony (Obstructive Disease)
Emergency Medicine Practice Question 1 — Auto-PEEP trigger failure
A ventilated COPD patient is taking visible inspiratory efforts but the ventilator fails to deliver assisted breaths. Which mechanism best explains this?
- A. Excessive external PEEP preventing exhalation
- B. Intrinsic PEEP requiring greater effort to drop airway pressure below trigger threshold
- C. Low FiO₂ causing hypoxic drive suppression
- D. High tidal volume causing alkalosis
- E. Inadequate humidification increasing secretions
Emergency Medicine Practice Question 2 — Best mode to improve synchrony (mechanism-based)
A child with severe asthma has frequent ventilator “bucking” despite appropriate sedation. Which mode most directly improves synchrony by using neural respiratory drive for triggering?
- A. NAVA
- B. SIMV
- C. Volume assist-control
- D. Pressure control ventilation
- E. CPAP only
Emergency Medicine Practice Question 3 — External PEEP in auto-PEEP
In an intubated asthmatic with suspected auto-PEEP and ineffective triggering, which adjustment can sometimes improve synchrony (when carefully applied)?
- A. Remove all PEEP (set PEEP to 0)
- B. Add low external PEEP titrated below measured intrinsic PEEP
- C. Increase respiratory rate to blow off CO₂
- D. Shorten expiratory time
- E. Increase I:E ratio to 2:1
Emergency Medicine Practice Question 4 — Ventilator strategy to reduce dynamic hyperinflation
Which ventilator setting strategy most helps minimize dynamic hyperinflation in severe asthma?
- A. High respiratory rate and short expiratory time
- B. Low respiratory rate with prolonged expiratory time
- C. High PEEP above intrinsic PEEP
- D. High tidal volume to “stent” airways open
- E. Inverse ratio ventilation
Emergency Medicine Practice Question 5 — Recognizing dyssynchrony consequence
A ventilated patient has severe dyssynchrony with double-triggering and high transpulmonary pressures. The main downstream risk is:
- A. Metabolic acidosis
- B. Ventilator-induced lung injury (barotrauma/volutrauma)
- C. Pulmonary embolism
- D. Aspiration pneumonia
- E. Cardiogenic pulmonary edema
Mini Case Discussion Prompt
Compare how you would address dyssynchrony in (1) intubated severe asthma with auto-PEEP versus (2) ARDS with high respiratory drive—what changes in preferred mode, sedation approach, and the role of external PEEP?
Mini-FAQ
Q1: Why does auto-PEEP cause missed triggers?
A: The patient must overcome intrinsic alveolar pressure before airway pressure/flow changes are detected; ABEM-style questions expect recognition of “ineffective triggering” in obstructive disease.
Q2: Is NAVA standard-of-care for intubated asthma?
A: Not universally; many guidelines emphasize lung-protective strategies and managing dynamic hyperinflation rather than mandating NAVA. Exams may still test NAVA as the mode that most directly improves synchrony when listed.
Q3: When can external PEEP help in obstructive disease?
A: When carefully titrated below intrinsic PEEP, it can reduce the inspiratory effort needed to trigger breaths; board questions often test this nuance.
Q4: What’s the board-facing priority in ventilating severe asthma?
A: Minimize dynamic hyperinflation (low rate, long expiratory time) and prevent VILI; mode matters less than settings and synchrony, unless the question explicitly asks for a mode.
Find this and other Emergency Medicine exam prep questions in Med-Challenger Emergency Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!