quick quiz
A 58-year-old woman presents to you with a 4-month history of postcoital spotting
It's Neoplasia Quiz Time with Med-Challenger!
NF1 is autosomal dominant with variable expressivity and frequent de novo mutations. Learn why this genetics question is commonly missed.
NF1 is classically autosomal dominant (often de novo), and boards expect you to distinguish this from X-linked and autosomal-recessive patterns.
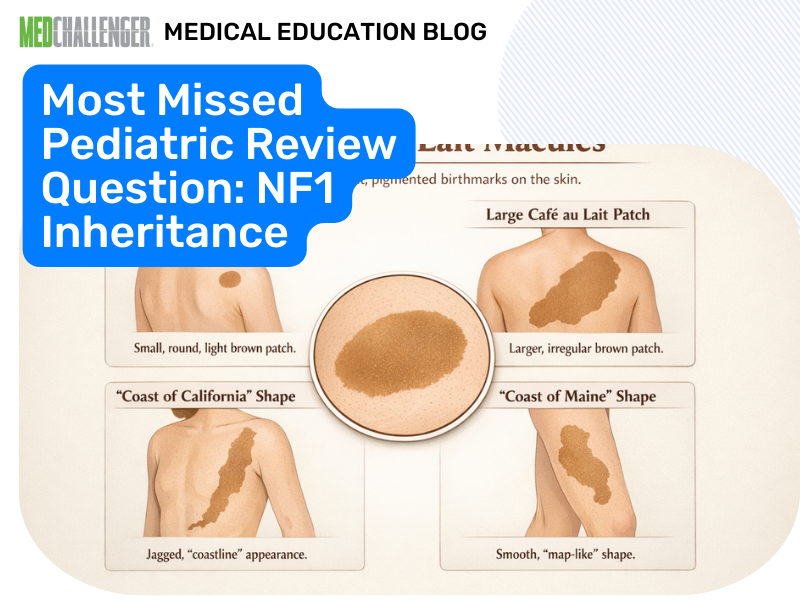
A 4-year-old girl has 7 cafe-au-lait macules over 5 mm in diameter scattered over her body and Lisch nodules on ophthalmic examination. You diagnose her with type 1 neurofibromatosis.

What is the inheritance pattern of this disorder?
Answer Options:
A. autosomal recessive
B. X-linked dominant
C. X-linked recessive
D. autosomal dominant
NF1 results from pathogenic variants in the NF1 tumor suppressor gene and is inherited in an autosomal-dominant pattern with variable expressivity. A major exam nuance is that many children have no family history because a substantial fraction of cases are de novo, but the inheritance pattern remains autosomal dominant.
This is consistent with modern, exam-relevant references including the American Academy of Pediatrics clinical report (2019) on health supervision in NF1 and GeneReviews (continually updated), both of which characterize NF1 as autosomal dominant.
- Confusion between NF1 vs NF2 features leads learners to overthink inheritance (both are AD, but presentations differ).
- De novo cases mislead test-takers into assuming autosomal recessive.
- “Café-au-lait” triggers memorized associations (e.g., McCune-Albright, tuberous sclerosis) instead of pattern recognition.
| Option | What It Tests / Implies | Why It’s Wrong Here |
|---|---|---|
| autosomal recessive | “No family history = recessive” heuristic | NF1 is autosomal dominant; lack of family history is commonly due to **de novo** mutation, not recessive inheritance. |
| X-linked dominant | Misattribution to sex-linked transmission | NF1 affects all sexes equally and is not classically transmitted via X-linked mechanisms. |
| X-linked recessive | Confusing with XLR neurocutaneous syndromes | NF1 is not XLR; XLR patterns skew heavily male and show carrier females—doesn’t fit. |
| autosomal dominant | Correct recognition of NF1 genetics | Correct; also high-yield: variable expressivity and frequent de novo cases. |
NF1 is autosomal dominant with variable expressivity and a high de novo mutation rate—don’t let “no family history” push you to autosomal recessive.
The stem gives classic diagnostic features (multiple café-au-lait macules >5 mm in a prepubertal child plus Lisch nodules) and then tests whether you can recall the inheritance pattern without being distracted by the possibility of absent family history—an exam-favorite trap.
A 6-year-old is diagnosed with NF1 and neither parent meets diagnostic criteria. What is the most accurate counseling point?
- A. The child’s condition is autosomal recessive
- B. The condition is autosomal dominant and may be due to a de novo mutation
- C. The condition is X-linked recessive
- D. Recurrence risk is zero for all future pregnancies
- E. Only males transmit the condition
A father with clinically apparent NF1 has one child. If the mother is unaffected, what is the approximate risk the child inherits the pathogenic variant?
- A. 0%
- B. 10%
- C. 25%
- D. 50%
- E. 100%
A child has multiple café-au-lait macules and axillary freckling. Which inheritance pattern best matches the most likely diagnosis?
- A. Autosomal recessive
- B. X-linked dominant
- C. X-linked recessive
- D. Autosomal dominant
- E. Mitochondrial
A woman with mild NF1 (few café-au-lait macules only) asks about severity in her future child if inherited. Best answer?
- A. Severity is always identical within a family
- B. Severity can vary widely due to variable expressivity
- C. Children will be unaffected if the parent is mildly affected
- D. Severity depends on whether the child is male
- E. Severity is predictable from the number of café-au-lait macules in the parent
Which gene category best describes NF1?
- A. Proto-oncogene
- B. Tumor suppressor gene
- C. Mismatch repair gene
- D. Mitochondrial gene
- E. Imprinting control gene
How would your genetic counseling differ for (1) a child with NF1 and unaffected parents versus (2) a child with NF1 and an affected parent—specifically regarding recurrence risk and the concept of mosaicism?
Q1: Does “no family history” change NF1 from autosomal dominant to something else?
A1: No. The ABP/board exams expect recognition that NF1 remains autosomal dominant and often arises de novo.
Q2: Are NF1 and NF2 inherited differently?
A2: No—both are classically autosomal dominant, but their hallmark clinical findings differ (boards test phenotype distinctions more than inheritance differences).
Q3: What single phrase best describes NF1 inheritance for exams?
A3: “Autosomal dominant with variable expressivity and frequent de novo mutations.”
Q4: Why do test writers include Lisch nodules in the stem?
A4: It anchors the diagnosis to NF1 so the inheritance question becomes a direct recall/recognition task—common on pediatrics boards.
Find this and other Pediatric Medicine exam prep questions in Med-Challenger Pediatric Medicine Exam Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!
/PEDS%20CHALLENGER.png?width=250&height=218&name=PEDS%20CHALLENGER.png)



No matter your program, no matter the size, Med-Challenger for Groups and Institutions can better prepare your program or group, fulfill industry requirements, and increase test scores.

It's Neoplasia Quiz Time with Med-Challenger!
It's Non-pruritic Rash Quiz Time with Med-Challenger!
Complete MyEMCert subscription now available on the new Med-Challenger FUSE LMS. Includes didactic topical review, case-based questions, and built-in...