abim
Addressing and Improving ABIM LKA Knowledge Gaps
The ABIM LKA is a continuous learning tool that can help physicians stay current and refine their skills.
Brugada type 1 ECG plus syncope is high risk. Learn why ICD—not Holter or observation—is the board-relevant next step per major guidelines.
When syncope occurs with a type 1 Brugada ECG pattern, the board-relevant next step is sudden-death prevention with an implantable cardioverter-defibrillator (ICD), not outpatient monitoring.

A 45-year-old man with a history of hypertension and diabetes mellitus presents to you for evaluation after a syncopal event earlier today. He is currently with no symptoms and notes no focal weakness or numbness. He takes hydrochlorothiazide for hypertension.
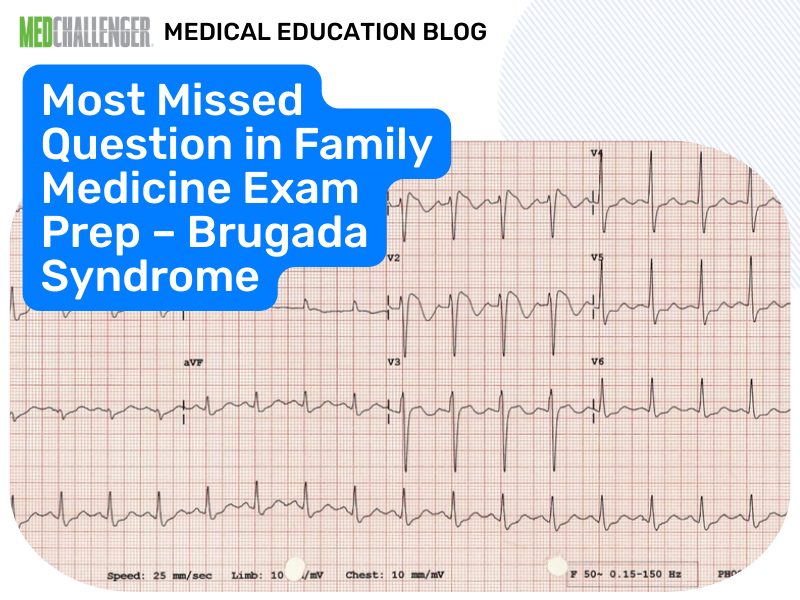
His blood pressure is 120/80 mm Hg and his pulse is 83 beats per minute. Findings on general physical and neurologic examinations are normal. Results from a complete blood count and basic metabolic panel are normal. A cardiac marker test is negative. Electrocardiography (ECG) is obtained (see Figure).
 Figure.
Figure.
What would be the best next step in the management of this patient's condition?
Answer Options:
This is a classic “ECG pattern + syncope” question. The provided remediation indicates the ECG demonstrates a Brugada type 1 pattern (coved ST-segment elevation in V1–V3 with subsequent T-wave inversion). In major guidelines (ESC 2022; ACC/AHA/HRS 2017), Brugada syndrome becomes high-stakes when paired with clinical events consistent with malignant ventricular arrhythmia—especially syncope that is unexplained and concerning for arrhythmic etiology. In that setting, the exam-reliable next step is ICD placement for prevention of sudden cardiac death.
Why this is frequently missed on boards: many test-takers treat “syncope” as a workup problem (Holter, echo, observation). But Brugada is fundamentally a sudden-death risk problem once symptomatic; monitoring may document arrhythmias but does not mitigate risk. Guidelines consistently emphasize ICD for secondary prevention and for symptomatic Brugada with arrhythmic syncope when the ECG pattern is type 1 and spontaneous/suggestive.
Guideline anchor:
| Option | What It Tests / Implies | Why It’s Wrong Here |
|---|---|---|
| implantation of a cardioverter defibrillator | Definitive SCD prevention in high-risk channelopathy | Correct: symptomatic Brugada (type 1 pattern + syncope concerning for arrhythmia) warrants ICD per major guidance. |
| observation | Low-risk syncope/benign ECG | Misses potentially lethal ventricular arrhythmia risk in Brugada syndrome. |
| echocardiography | Structural heart disease evaluation | Brugada is primarily an electrical/channelopathy diagnosis; echo may be adjunctive but is not the best “next step” for risk mitigation. |
| Holter monitor | Ambulatory rhythm documentation | May fail to capture intermittent polymorphic VT/VF and does not prevent SCD; not the best next step in a high-risk Brugada presentation. |
In type 1 Brugada pattern with syncope suspicious for arrhythmia, choose CD over outpatient monitoring.
The stem distracts you with normal vitals, normal labs, and negative troponin to prompt a “reassurance/monitoring” reflex. Boards reward pattern recognition: when the ECG suggests Brugada and the patient has syncope compatible with arrhythmia, the next step is sudden death prevention, not incremental diagnostics.
A 38-year-old man is found to have a Brugada-like ECG pattern during a pre-op evaluation. He has never had syncope, seizures, or palpitations. No family history of sudden death. What is the most appropriate management?
A 29-year-old man develops fever from influenza and has an ECG showing coved ST elevation in V1–V2 consistent with type 1 Brugada pattern. He reports near-syncope while febrile but is now stable. Best immediate step?
A 46-year-old man with spontaneous type 1 Brugada ECG survives an out-of-hospital cardiac arrest with documented VF. Next step for secondary prevention?
A 52-year-old woman has syncope after prolonged standing in a hot room, with prodrome (nausea, diaphoresis). ECG normal. Best next step?
A 41-year-old man has coved ST elevation in V1–V2 with negative T waves. He is afebrile, chest-pain free, and troponin is negative. He had unexplained syncope while watching TV. Most appropriate management plan?
How would your management change between (1) an incidental Brugada pattern found on ECG, (2) type 1 pattern with fever only, and (3) type 1 pattern with unexplained syncope?
A: Boards expect you to pair a diagnostic ECG (typically type 1) with clinical criteria such as syncope or documented VT/VF—this shifts management toward SCD prevention.
A: ABIM/board-style questions treat symptomatic Brugada as a malignant ventricular arrhythmia risk; Holter may miss intermittent VF/PMVT and doesn’t prevent sudden death.
A: After cardiac arrest/VT/VF (secondary prevention) and in high-risk symptomatic patients (e.g., syncope likely arrhythmic with spontaneous type 1 pattern), consistent with ACC/AHA/HRS 2017 and ESC 2022 risk-based guidance.
A: Fever—test writers frequently use febrile illness to unmask type 1 pattern; prompt antipyresis and escalation are expected.
Find this and other Family Medicine exam prep questions in Med-Challenger Family Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!



No matter your program, no matter the size, Med-Challenger for Groups and Institutions can better prepare your program or group, fulfill industry requirements, and increase test scores.

The ABIM LKA is a continuous learning tool that can help physicians stay current and refine their skills.
Complete MyEMCert subscription now available on the new Med-Challenger FUSE LMS. Includes didactic topical review, case-based questions, and built-in...
DEA moves to reclassify marijuana, fulfill MOC needs, providers have questions regarding AI and patient care, and nursing program enrollment down