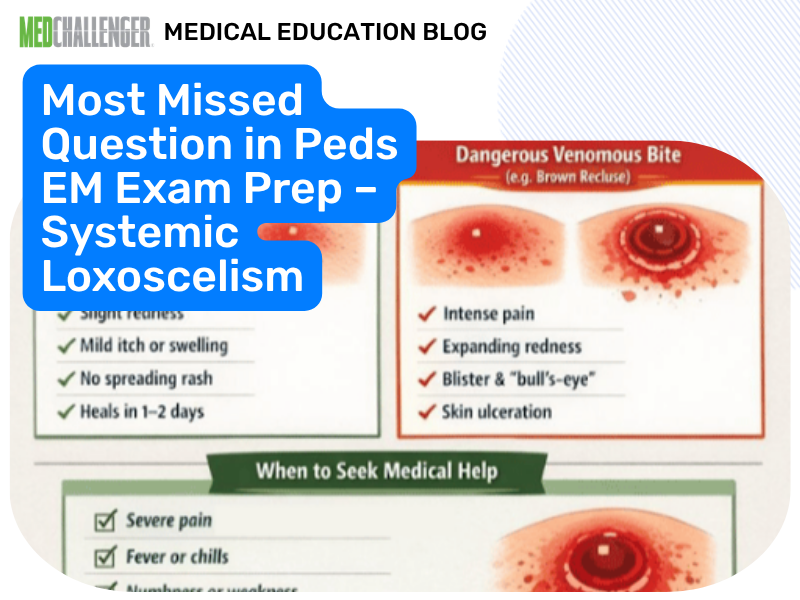
Systemic brown recluse envenomation in children can present with “flu-like” symptoms followed by hemolysis and DIC—an exam-favorite pattern recognition task.
Question – Envenomation ID
A 12-month-old boy presents to the ED after developing flu-like symptoms. Parents noted fever, chills, nausea and vomiting, and weakness. On examination, you notice petechiae. Laboratory findings demonstrate acute hemolysis, DIC, and rhabdomyolysis.
Which envenomation can lead to these complications?
Answer Options:
A. Agkistrodon (copperhead)
B. Heloderma horridum (beaded lizard)
C. Loxosceles (brown recluse)
D. Megalopyge (puss caterpillar)
The keyed answer (Loxosceles) is consistent with current exam-relevant consensus: systemic loxoscelism can cause delayed constitutional symptoms and severe systemic toxicity including intravascular hemolysis and DIC, particularly in pediatric patients (Wilderness Medical Society Practice Guidelines, 2016; Goldfrank’s Toxicologic Emergencies, 2019). Petechiae in this stem fits DIC/thrombocytopenia physiology. Rhabdomyolysis is less “signature” than hemolysis/DIC but is described among severe systemic toxic effects in case-based toxicology literature and is compatible with a severe systemic envenomation illness script.
Boards often test that brown recluse is not only a necrotic wound: the high-risk, time-delayed systemic syndrome (often 24–72+ hours after bite) is the key discriminator.
Why This Pediatric Emergency Medicine Question Is Often Missed
- Test-takers over-anchor on the necrotic skin lesion and miss that children can develop systemic hemolysis/DIC.
- The stem mimics sepsis/meningococcemia (flu-like + petechiae), but the question asks specifically for envenomation.
- Copperhead/rattlesnake are incorrectly generalized to “any venom can cause DIC/hemolysis.”
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| Agkistrodon (copperhead) |
Pit viper envenomation → coagulopathy, local tissue injury |
Copperhead bites are typically less severe; while pit vipers can cause coagulopathy, this stem’s hemolysis + DIC pattern is classically tested with loxoscelism rather than copperhead. |
| Heloderma horridum (beaded lizard) |
Venomous lizard bite |
Typically causes local pain, edema, and systemic symptoms (e.g., hypotension) are uncommon; not the classic hemolysis/DIC syndrome in boards. |
| Loxosceles (brown recluse) |
Systemic loxoscelism |
Best match: delayed flu-like symptoms with intravascular hemolysis and DIC, especially in children (WMS 2016; Goldfrank 2019). |
| Megalopyge (puss caterpillar) |
Caterpillar setae toxin dermatitis |
Causes localized pain/dermatitis; does not cause hemolysis/DIC/rhabdomyolysis. |
High-Yield Pearl for Exam Prep
In a child with delayed “flu-like” illness plus hemolysis and DIC, think systemic loxoscelism (brown recluse) even if a dramatic necrotic lesion is not emphasized.
Core Learning Objectives
- Identify the clinical syndrome of systemic loxoscelism, including delayed constitutional symptoms with hemolysis and DIC in pediatric patients.
- Differentiate systemic loxoscelism from other common envenomations that primarily cause local reactions or different systemic toxidromes.
The Exam “Test Trick” at Play
This item rewards syndrome recognition: “flu-like prodrome + petechiae + hemolysis/DIC” points to toxin-mediated hematologic catastrophe rather than a purely local bite reaction. The distractors are “well-known” exposures, but only one is consistently associated with delayed hemolysis/DIC on exams.
Additional Peds EM Practice Questions and Remediation for Loxosceles Envenomation
Pediatric Emergency Medicine Practice Question 1 — Delayed hemolysis
A 6-year-old develops fever, malaise, and dark urine 48 hours after a suspected spider bite. Labs show falling hemoglobin, elevated LDH, and indirect hyperbilirubinemia. What is the most likely culprit?
- A. Latrodectus (black widow)
- B. Loxosceles (brown recluse)
- C. Tityus (scorpion)
- D. Agkistrodon contortrix (copperhead)
- E. Megalopyge (puss caterpillar)
Pediatric Emergency Medicine Practice Question 2 - Board-relevant complication
Which complication is most classically associated with systemic loxoscelism in children?
- A. Myasthenic crisis
- B. Disseminated intravascular coagulation
- C. Flaccid paralysis from botulinum toxin
- D. Symmetric ascending paralysis (GBS)
- E. Acute pancreatitis
Pediatric Emergency Medicine Practice Question 3 - Best differentiator
A teen presents with severe muscle cramping, abdominal pain, diaphoresis, and hypertension after a spider bite; labs show no hemolysis. Which is most likely?
- A. Latrodectus (black widow)
- B. Loxosceles (brown recluse)
- C. Megalopyge (puss caterpillar)
- D. Heloderma horridum (beaded lizard)
- E. Agkistrodon (copperhead)
Pediatric Emergency Medicine Practice Question 4 - Management emphasis
A 4-year-old with suspected systemic loxoscelism has hemoglobin drop and signs of coagulopathy. Best next step in ED management?
- A. Immediate dapsone for all patients
- B. Supportive care with close monitoring and treatment of hemolysis/DIC as indicated
- C. Prophylactic antibiotics to prevent necrosis
- D. Immediate surgical excision of the bite site
- E. Hyperbaric oxygen as first-line therapy
Pediatric Emergency Medicine Practice Question 5 - Local vs systemic
A patient has immediate burning pain and erythematous papules in a “tram-track” pattern after contact with a fuzzy caterpillar; no systemic abnormalities. Most likely exposure?
- A. Loxosceles (brown recluse)
- B. Agkistrodon (copperhead)
- C. Megalopyge (puss caterpillar)
- D. Heloderma horridum (beaded lizard)
- E. Latrodectus (black widow)
Mini Case Discussion Prompt
How would you distinguish systemic loxoscelism from meningococcemia or other septic petechial illnesses in a child when the history of a bite is uncertain, and what minimum lab monitoring would you order?
Mini-FAQ
Q1: What is the single most board-relevant systemic complication of brown recluse bite in children?
A: Hemolysis with possible DIC; the ABIM/ABP-style framing expects recognition of delayed intravascular hemolysis rather than only a necrotic lesion (WMS 2016).
Q2: Does every brown recluse bite cause skin necrosis?
A: No. Many are mild; boards test that systemic loxoscelism can occur even when the skin findings are not dramatic.
Q3: Is dapsone standard therapy for brown recluse bites?
A: No. Contemporary guidance emphasizes supportive care; dapsone is not routine due to limited evidence and adverse effects (WMS 2016).
Q4: What “look-alike” toxidrome should you contrast with loxoscelism?
A: Latrodectism (black widow)—prominent muscle cramps and autonomic symptoms without the hemolysis/DIC pattern.
Find this and other Pediatric Emergency Medicine exam prep questions in Med-Challenger Pediatric Emergency Medicine 3rd Edition Exam Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements.