Key takeaway: In febrile children with a benign abdominal exam, right lower-lobe pneumonia is a classic cause of RUQ abdominal pain—obtain a chest radiograph when suspected.
Question - RUQ pain with fever
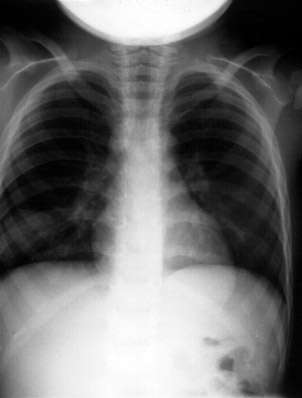
This child presented with complaints of fever and RUQ abdominal pain. The abdominal exam was benign. What's causing the upper abdominal pain?

Answer Options:
A. subhepatic abscess
B. ruptured viscus
C. pneumonia
D. pneumothorax
E. pneumoperitoneum
This high-miss item tests recognition that lower-lobe pneumonia can present with abdominal pain, particularly RUQ pain, in children due to diaphragmatic irritation and shared innervation. A benign abdominal exam with fever should prompt consideration of chest pathology, and CXR often reveals a basilar infiltrate.
The keyed answer (pneumonia) is correct and guideline-concordant. ACR Appropriateness Criteria (2023) for suspected appendicitis in children explicitly notes pneumonia as an extra-abdominal cause of abdominal pain and supports chest imaging when clinical features suggest it. AAP Pediatrics in Review (2021) likewise emphasizes lower-lobe pneumonia as a common mimic of acute abdomen in pediatrics.
Why This Emergency Medicine Question Is Often Missed
- Anchoring on abdominal etiologies (e.g., appendicitis, hepatobiliary disease) despite a benign abdominal exam.
- Failure to consider referred pain from the chest in febrile children.
- Underuse of chest radiography in pediatric abdominal pain when respiratory or systemic clues exist.
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| subhepatic abscess |
Deep intra-abdominal infection post-appendicitis/hepatobiliary source |
Would typically have peritoneal signs, systemic toxicity, or imaging evidence; benign abdominal exam argues against. |
| ruptured viscus |
Perforation/peritonitis recognition |
Would present with acute abdomen, guarding/rigidity, free air; benign exam contradicts. |
| pneumonia |
Recognition of extra-abdominal cause of abdominal pain |
Correct: Lower-lobe pneumonia commonly causes RUQ pain in children; CXR shows basilar infiltrate. |
| pneumothorax |
Thoracic cause with pleuritic pain/dyspnea, decreased breath sounds |
Localizes to chest symptoms; does not typically cause isolated RUQ abdominal pain and CXR pattern would differ. |
| pneumoperitoneum |
Free intraperitoneal air from perforation |
Would have peritoneal signs; upright CXR would show subdiaphragmatic free air, not basilar consolidation. |
High-Yield Pearl for ABEM Exam Prep
In a febrile child with RUQ or right lower quadrant pain and a benign abdominal exam, always consider and image for right lower-lobe pneumonia.
Core Learning Objectives
1. Recognize lower-lobe pneumonia as a common extra-abdominal cause of pediatric abdominal pain.
2. Select appropriate diagnostic imaging (chest radiography) when clinical features suggest chest pathology despite a benign abdominal exam.
The Exam Trick at Play
This item probes failure to broaden the differential: abdominal pain does not always equal abdominal pathology—particularly in pediatrics, where lower-lobe pneumonias frequently masquerade as acute abdomen.
Additional Practice Questions & Remediation for Abdominal Pain Mimics
Emergency Medicine Practice Question 1 — Febrile RUQ pain, normal abdomen
A 7-year-old has fever, cough, and RUQ pain; abdomen is soft and non-tender. Next best test?
A. Abdominal CT with contrast
B. Chest radiograph
C. Abdominal ultrasound
D. Serum lipase
E. Diagnostic laparoscopy
Emergency Medicine Practice Question 2 — RLQ pain mimic
A 9-year-old with fever and right lower quadrant pain, mild tachypnea, no guarding; coarse crackles at right base. Most likely diagnosis?
A. Appendicitis
B. Mesenteric adenitis
C. Right lower-lobe pneumonia
D. Cholecystitis
E. Intussusception
Emergency Medicine Practice Question 3 — Imaging pathway
A 6-year-old with fever and vague periumbilical pain; clear lungs on auscultation but pleuritic cough and O2 sat 93%; abdomen benign. Best initial imaging?
A. PA and lateral chest radiograph
B. Right upper quadrant ultrasound
C. KUB radiograph
D. CT abdomen/pelvis with IV contrast
E. No imaging; discharge
Emergency Medicine Practice Question 4 — When abdomen is not the source
Which feature most increases pretest probability that a child’s abdominal pain is from pneumonia?
A. Pain worsens after eating
B. Bilious emesis
C. Fever with cough and benign abdominal exam
D. Localized rebound tenderness
E. Pain relieved by bowel movement
Emergency Medicine Practice Question 5 — Avoiding missed pneumonia
A 5-year-old presents with isolated RUQ pain and fever; no cough reported. Lungs clear; abdomen benign. Next best step?
A. Immediate abdominal CT
B. Observe without imaging
C. Obtain chest radiograph
D. Start broad-spectrum IV antibiotics and admit
E. Discharge with return precautions only
Mini Case Discussion Prompt
Compare two children with RUQ pain and fever: one with overt cough and hypoxemia versus one without respiratory complaints and clear lungs. How do pretest probabilities for pneumonia differ, and how does this change your threshold for ordering CXR versus abdominal imaging?
Mini-FAQ
- Q: Why does lower-lobe pneumonia cause abdominal pain in children?
A: Diaphragmatic and parietal pleura irritation refers pain to the abdomen via shared innervation—boards expect recognition of this mimic.
- Q: When should I order a chest radiograph for pediatric abdominal pain?
A: In febrile children with benign abdominal exam and any respiratory features (cough, tachypnea, hypoxemia) or right-sided abdominal pain—per ACR (2023).
- Q: Can auscultation be normal in basilar pneumonia?
A: Yes; physical findings may be subtle. A low threshold for CXR is testable high-yield.
- Q: Do guidelines support avoiding abdominal CT initially?
A: Yes; ACR (2023) emphasizes minimizing radiation and targeting imaging to likely pathology—start with CXR when pneumonia is suspected.
Find this and other Emergency Medicine exam prep questions in Med-Challenger Emergency Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!






