Severe primary hypothyroidism can produce a sellar mass–appearing pituitary enlargement via TRH-driven pituitary hyperplasia, and the labs (very high TSH + low free T4) make the diagnosis.
Question – Sellar mass
A 32-year-old man with no previous medical history complains of frontal headache for 3 months, unintentional weight gain of 10 pounds, and cold intolerance. On examination, his blood pressure is 120/60 mm Hg and his pulse is 60 beats/minute. His thyroid is not enlarged. His thyroid-stimulating hormone (TSH) level is 464 mIU/L (normal range, 2.5-4.0 mIU/L), free thyroxine (T4) is 0.1 ng/dL (normal range, 0.7-1.9 ng/dL), and free triiodothyronine (T3) is 75 pg/dL (normal range, 230-619 pg/dL).Magnetic resonance imaging of the brain shows a sellar mass extending into the suprasellar cistern with mild compression of the optic chiasm (see Figure).
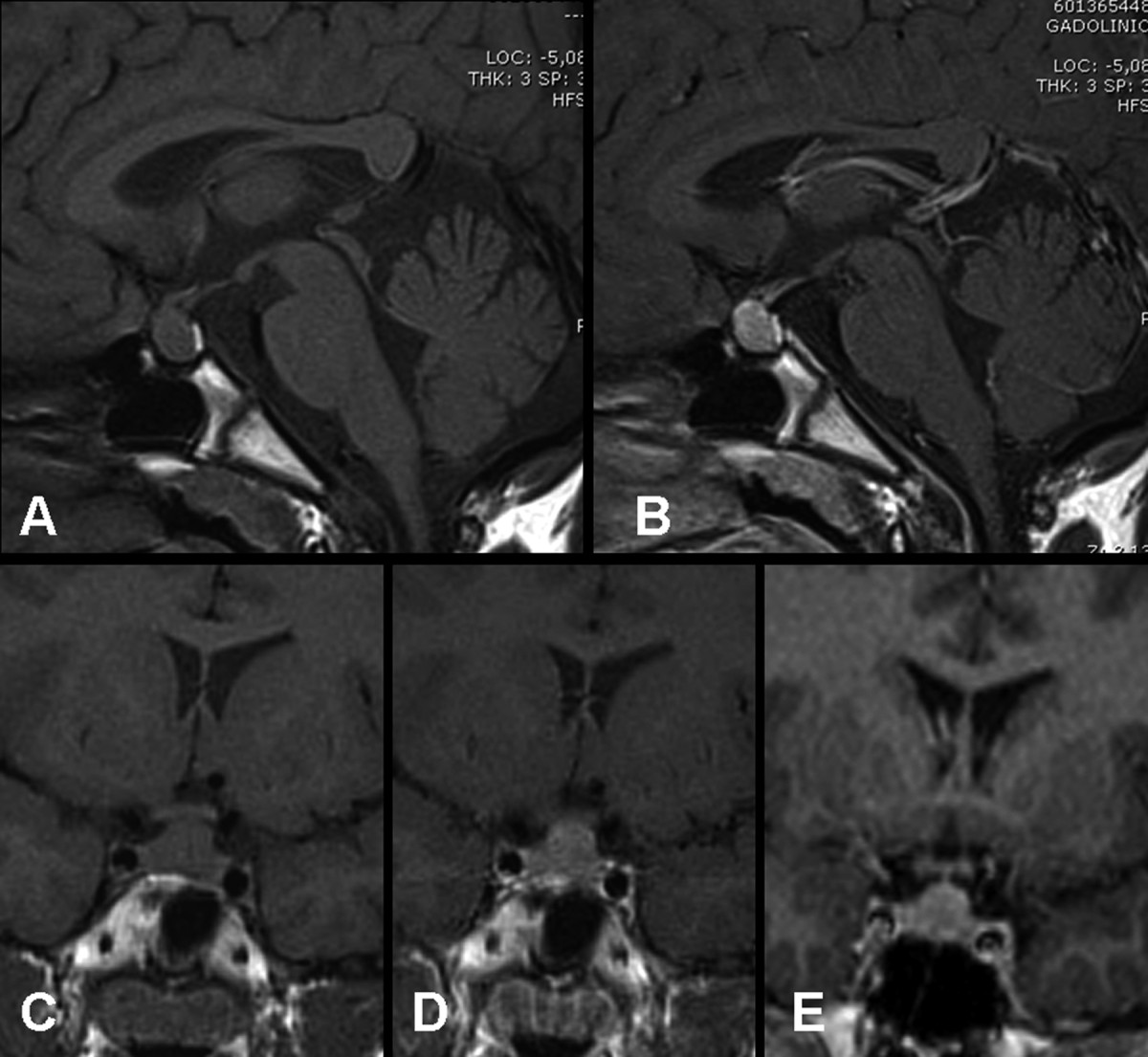 Figure. Reproduced from Franceschi R, Rozzanigo U, Failo R, Bellizzi M, Di Palma A. Pituitary hyperplasia secondary to acquired hypothyroidism: case report. Ital J Pediatr. 2011;37:15.
Figure. Reproduced from Franceschi R, Rozzanigo U, Failo R, Bellizzi M, Di Palma A. Pituitary hyperplasia secondary to acquired hypothyroidism: case report. Ital J Pediatr. 2011;37:15.
What is the likely cause of this patient’s sellar mass?
Answer Options:
A. TSH-producing adenoma
B. hypothalamic lesions
C. primary hypothyroidism
D. nonsecreting pituitary adenoma
This keyed answer is correct by current standard endocrine diagnostic principles: the biochemical profile (TSH 464 mIU/L with profoundly low free T4/T3) is unequivocal primary hypothyroidism. In severe, prolonged primary hypothyroidism, loss of negative feedback increases hypothalamic TRH, which can drive pituitary thyrotroph hyperplasia (and often lactotroph hyperplasia), producing apparent pituitary “macroadenoma” imaging findings and mass-effect symptoms (e.g., headache, chiasmal compression).
This is a classic board trap: test-takers anchor on “sellar mass = pituitary adenoma” and ignore the thyroid axis pattern. Major guidance (e.g., ATA hypothyroidism guidance and Endocrine Society hypopituitarism guidance) reinforces that primary hypothyroidism is defined by high TSH with low free T4, whereas pituitary (central) etiologies more often show low or inappropriately normal TSH with low free T4.
Why This Family Medicine Question Is Frequently Missed
- “Mass on MRI” triggers reflex selection of pituitary adenoma despite thyroid labs that strongly localize disease to the thyroid gland.
- Confusion between TSH-secreting adenoma (high TSH *and* high T4/T3) vs primary hypothyroidism (high TSH with low T4/T3).
- Under-recognition that pituitary enlargement can be reactive hyperplasia and may regress with levothyroxine.
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| TSH-producing adenoma |
Secondary hyperthyroidism due to TSHoma |
TSHomas classically have **elevated/unsuppressed TSH with elevated free T4/T3**, not profoundly low T4/T3. |
| hypothalamic lesions |
Tertiary hypothyroidism or hypothalamic mass effect |
A hypothalamic process would not typically present as a **sellar** mass, and thyroid labs in central causes are usually **low free T4 with low/normal TSH**, not TSH 464. |
| primary hypothyroidism |
Loss of thyroid hormone → ↑TSH/↑TRH |
Fits perfectly: **very high TSH + very low free T4/T3**, plus pituitary hyperplasia can mimic macroadenoma on MRI. |
| nonsecreting pituitary adenoma |
Mass effect with hypopituitarism |
Would more often cause **central hypothyroidism** (low free T4 with **low/inappropriately normal TSH**), not extreme TSH elevation. |
High-Yield Pearl for Family Medicine Exam Prep
A “pituitary macroadenoma” on MRI plus TSH in the hundreds with low free T4 is severe primary hypothyroidism with pituitary hyperplasia until proven otherwise.
Core Learning Objectives
1. Differentiate primary hypothyroidism from central hypothyroidism and TSH-secreting adenoma using TSH and free T4/T3 patterns.
2. Recognize that severe primary hypothyroidism can cause pituitary hyperplasia that mimics a sellar mass and may regress with thyroid hormone replacement.
The “Test Trick” at Play
The stem supplies everything needed to localize pathology to the thyroid (massive TSH elevation with very low free T4/T3), but then introduces an MRI “mass” to bait a pituitary tumor diagnosis. Boards reward prioritizing physiology and axis logic over imaging anchoring—especially when the lab pattern is pathognomonic.
Additional FM Practice Questions and Remediation for Pituitary Hyperplasia
Family Medicine Practice Question 1 - TSHoma vs primary
A 45-year-old has palpitations and weight loss. TSH is 6.2 mIU/L (high), free T4 is 3.1 ng/dL (high). MRI shows a pituitary lesion. Most likely diagnosis?
A. Primary hypothyroidism
B. TSH-secreting pituitary adenoma
C. Nonfunctioning pituitary adenoma with stalk effect
D. Secondary (central) hypothyroidism
E. Subacute thyroiditis
Family Medicine Practice Question 2 - Central hypothyroidism pattern
A 52-year-old with known pituitary macroadenoma has fatigue. Free T4 is low; TSH is 1.1 (normal). Best interpretation?
A. Primary hypothyroidism
B. Central (secondary) hypothyroidism
C. TSH-secreting adenoma
D. Euthyroid sick syndrome
E. Graves disease
Family Medicine Practice Question 3 - Sellar enlargement in hypothyroidism
A 28-year-old postpartum patient has weight gain, constipation, and headaches. TSH 210, free T4 very low. MRI shows diffuse pituitary enlargement. Best next step?
A. Transsphenoidal surgery
B. Start levothyroxine and repeat pituitary imaging after endocrine stabilization
C. Start methimazole
D. Start dopamine agonist immediately as first-line
E. Start high-dose glucocorticoids for suspected hypophysitis without further workup
Family Medicine Practice Question 4 - Stalk effect vs hyperplasia
A 40-year-old has mild hyperprolactinemia and headaches. Free T4 low, TSH low. MRI shows a nonfunctioning macroadenoma. Mechanism of hypothyroidism?
A. Primary thyroid failure
B. TRH-driven thyrotroph hyperplasia
C. Central hypothyroidism from pituitary compression
D. TSHoma secretion
E. Thyroid hormone resistance
Family Medicine Practice Question 5 - Board-style localization
A patient has cold intolerance. TSH 95 (high), free T4 low. No goiter. What does this localize?
A. Thyroid gland (primary hypothyroidism)
B. Pituitary gland (secondary hypothyroidism)
C. Hypothalamus (tertiary hypothyroidism)
D. Peripheral deiodinase defect
E. Assay interference is most likely
Mini Case Discussion Prompt
How would your differential and first management step change if the MRI showed a similar sellar mass but the labs were low free T4 with low/normal TSH instead of markedly elevated TSH?
Mini-FAQ
Q1: Why doesn’t a pituitary mass automatically mean “central hypothyroidism”?
A: Boards expect you to prioritize axis physiology: central hypothyroidism typically has low free T4 with low/inappropriately normal TSH, not TSH in the hundreds.
Q2: What lab pattern points to a TSH-secreting adenoma?
A: High free T4/T3 with non-suppressed or elevated TSH; ABFM-style questions often use this to distinguish TSHoma from primary hypothyroidism.
Q3: Can primary hypothyroidism really enlarge the pituitary?
A: Yes—severe, prolonged primary hypothyroidism can increase TRH drive and cause pituitary hyperplasia that mimics adenoma on imaging and may regress with levothyroxine.
Q4: What is the exam-reliable “first move” when severe primary hypothyroidism explains the picture?
A: Treat with levothyroxine and reassess; surgery is not first-line when imaging findings are consistent with reactive hyperplasia and the thyroid axis is diagnostic.
Find this and other Family Medicine exam prep questions in Med-Challenger Family Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!

No matter your program, no matter the size, Med-Challenger for Groups and Institutions can better prepare your program or group, fulfill industry requirements, and increase test scores.
For personal medical education that includes board's prep, MOC, and CME requirements, Med-Challenger has you covered in Family Medicine, Emergency Medicine, Internal Medicine, Pediatrics, Pediatric Emergency Medicine, OBGYN, Physician Assistants, and Nurse Practitioners.
Never miss a thing. Subscribe to our blog and save!