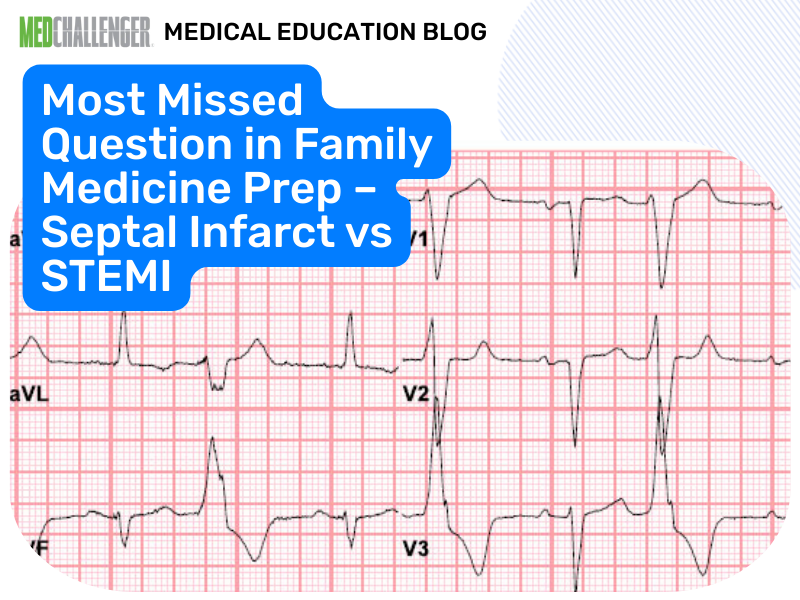
ECG evidence of pathologic septal Q waves/QS in V1–V2 supports a prior septal infarct (age indeterminate) rather than acute STEMI, digoxin effect, or PE strain.
Question – ECG Diagnosis
An 82-year-old man living in a nursing home presents to you with extreme shortness of breath. He denies having chest pain and has no history of coronary artery disease. His history includes gastroesophageal reflux disease (patient is taking omeprazole), type 2 diabetes mellitus (patient is taking glargine and metformin), hypertension (patient is taking lisinopril and hydrochlorothiazide), congestive heart failure (patient is taking digitalis), and Alzheimer dementia (patient is taking donepezil and memantine).
On examination, he has some rales at both lung bases, 3+ pitting edema of both feet and ankles, with some tenderness in both calves. There is a small diabetic ulcer on his right heel with a black eschar and some surrounding erythema. There appears to be right-upper quadrant tenderness and hepatomegaly. As part of his workup, you obtain electrocardiography (ECG; see Figure).
 Figure.
Figure.
What is your diagnosis?
Answer Options:
A. acute anterior ST elevation myocardial infarction (STEMI)
B. acute posterior ST elevation myocardial infarction (STEMI)
C. septal infarct of indeterminate age
D. digitalis effect
E. acute pulmonary embolism with right heart strain
In this item, the keyed answer (C) is reasonable and consistent with modern ECG interpretation, but the database remediation is incomplete because it does not anchor the interpretation to contemporary definitions of infarction patterns (and it over-emphasizes “dating” an infarct from ECG alone).
Boards commonly test that pathologic Q waves (or QS complexes) in V1–V2 indicate septal infarction (often prior), whereas acute STEMI requires *acute ischemic ST-segment changes in a consistent lead distribution* plus clinical context. The Fourth Universal Definition of MI (ESC/ACC/AHA/WHF, 2018) supports using pathologic Q waves as evidence of myocardial infarction (often prior), but ECG alone cannot reliably establish timing—hence “indeterminate age.”
Why This Family Medicine Question Is Frequently Missed
- The stem’s dyspnea + calf tenderness + edema pushes test-takers toward PE, even though classic PE ECG findings are neither sensitive nor specific.
- “Digitalis” in the med list triggers anchoring on digoxin effect, but digoxin effect is primarily ST-segment “scooping” and related repolarization changes—not isolated septal Q waves.
- Learners confuse Q waves (prior infarct marker) with acute STEMI criteria (ST elevation in a coronary territory).
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| A. acute anterior STEMI |
Looks for ST elevation in V1–V4 (± reciprocal changes) |
Pathologic Q/QS in V1–V2 without convincing acute STE pattern is more consistent with prior septal infarct than acute anterior STEMI. |
| B. acute posterior STEMI |
Expects ST depression + tall R waves in V1–V3; confirm with posterior leads V7–V9 |
Septal Q/QS pattern is not the classic posterior MI pattern (posterior MI gives **tall R** in V1–V2, not deep Q). |
| C. septal infarct of indeterminate age |
Recognizes Q waves/QS in V1–V2 as prior septal infarct |
Best match to the described ECG interpretation target. |
| D. digitalis effect |
“Scooped” downsloping ST depression, shortened QT (often), toxic rhythms if overdose |
Digoxin effect does not present as isolated septal Q waves; also QT prolongation is **not** a typical digoxin effect (digoxin more often shortens QT via shortened ventricular AP). |
| E. acute PE with right heart strain |
Sinus tachy, RBBB, right axis deviation, T inversions V1–V4, S1Q3T3 |
These are nonspecific and not described as the key ECG abnormality; PE cannot be diagnosed from ECG alone. |
High-Yield Pearl for Family Medicine Exam Prep
Pathologic Q waves/QS in V1–V2 = think septal infarct (often old); acute STEMI requires acute ST-segment criteria in a vascular territory.
Core Learning Objectives
1. Recognize ECG patterns consistent with prior septal infarction (pathologic Q waves/QS in V1–V2) versus acute STEMI patterns.
2. Distinguish digoxin effect and PE right-heart strain ECG clues from infarction patterns, and understand their diagnostic limitations.
The “Test Trick” at Play
The stem provides multiple “clinical lures” (dyspnea, calf tenderness, digoxin use) to bait you into diagnosing PE strain or digoxin effect. The board-style move is to answer the question that was asked—“What is your diagnosis?” based on the ECG pattern—and not to over-weight the clinical narrative when the prompt is explicitly testing ECG recognition.
Additional FM Practice Questions and Remediation for Septal Infarct on ECG
Family Medicine Practice Question 1 - Septal Q waves
A 64-year-old man is asymptomatic at a pre-op visit. ECG shows QS complexes in V1–V2 with normal ST segments and T waves. Most likely interpretation?
- A. Acute anterior STEMI
- B. Acute posterior STEMI
- C. Prior septal infarct (age indeterminate)
- D. Acute pericarditis
- E. Hyperkalemia
Family Medicine Practice Question 2 - Posterior MI confirmation
ECG shows horizontal ST depression in V1–V3 with tall R waves in V2. Best next step to confirm suspected posterior MI?
- A. Right-sided leads V3R–V4R
- B. Posterior leads V7–V9
- C. Repeat ECG in 24 hours only
- D. Adenosine challenge
- E. Carotid sinus massage
Family Medicine Practice Question 3 - Digoxin effect vs ischemia
A patient on digoxin has ECG with “scooped” downsloping ST depression in lateral leads and a shortened QT interval. Best interpretation?
- A. Acute lateral STEMI
- B. Digoxin effect
- C. Hypercalcemia
- D. Acute PE with right heart strain
- E. Brugada syndrome
Family Medicine Practice Question 4 - PE strain pattern limitation
Which ECG finding is most associated with acute PE with right ventricular strain (though not diagnostic)?
- A. Diffuse ST elevation
- B. Pathologic Q waves in V1–V2
- C. T-wave inversions in V1–V4 (right precordial) ± incomplete RBBB
- D. New LBBB with concordant ST elevation
- E. Prominent U waves
Family Medicine Practice Question 5 - Acute anterior STEMI criteria
A 58-year-old has crushing chest pain. ECG shows ST elevation in V2–V4 with reciprocal ST depression in II, III, aVF. Best diagnosis?
- A. Acute anterior STEMI
- B. Prior septal infarct only
- C. Acute pericarditis
- D. Early repolarization
- E. Digoxin effect
Mini Case Discussion Prompt
How would your differential and immediate workup change if this patient’s ECG instead showed sinus tachycardia with new RBBB and T-wave inversions V1–V4, and bedside ultrasound demonstrated RV dilation?
Mini-FAQ
Q1: Can you determine “age” of an infarct from ECG Q waves?
A: The ABFM/ABIM generally expects recognition that Q waves suggest prior infarction, but timing is often indeterminate without prior ECGs/biomarkers (Fourth Universal Definition of MI, 2018).
Q2: What’s the fastest way to separate posterior MI from septal Q waves on exam day?
A: Posterior MI typically shows ST depression + tall R in V1–V3; septal infarct shows Q/QS in V1–V2.
Q3: What are the classic “digoxin effect” ECG changes?
A: “Scooped” ST depression, T-wave changes, and sometimes shortened QT; toxicity more often causes arrhythmias (e.g., atrial tachycardia with block) than isolated Q waves.
Q4: Does an ECG diagnose pulmonary embolism?
A: No—ECG findings are supportive at best. The boards test that PE is a clinical/imaging diagnosis, with ECG used to assess strain and exclude mimics.
Find this and other Family Medicine exam prep questions in Med-Challenger Family Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!

No matter your program, no matter the size, Med-Challenger for Groups and Institutions can better prepare your program or group, fulfill industry requirements, and increase test scores.
For personal medical education that includes board's prep, MOC, and CME requirements, Med-Challenger has you covered in Family Medicine, Emergency Medicine, Internal Medicine, Pediatrics, Pediatric Emergency Medicine, OBGYN, Physician Assistants, and Nurse Practitioners.
Never miss a thing. Subscribe to our blog and save!