emergency medicine
43-year-old man with a prior history of an open appendectomy presents with vomiting, abdominal pain, and distension
It's Open Appendectomy Quiz Time with Med-Challenger!
It's Gastro Disorders Quiz Time with Med-Challenger!
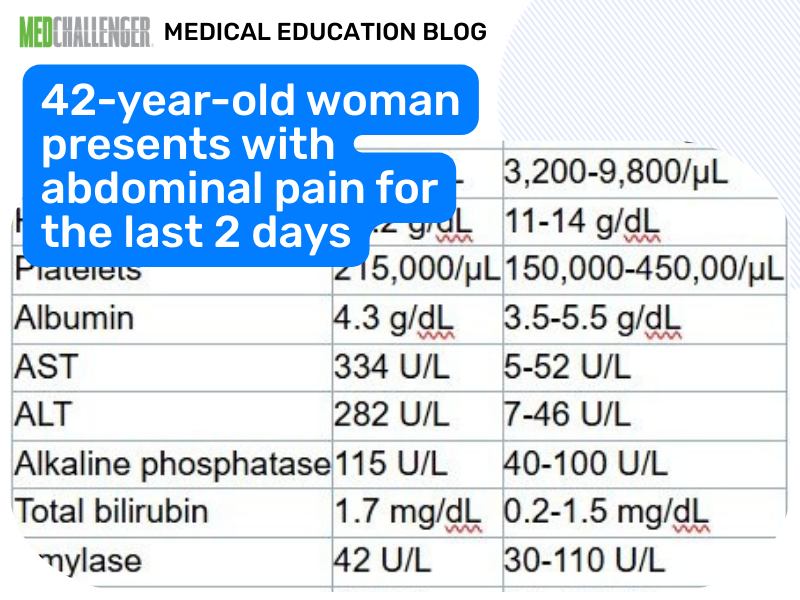
A 42-year-old woman presents with abdominal pain for the last 2 days. She describes the pain as crampy and intermittent in the epigastric area, and she tells you that it is particularly worse after meals. She has a history of Roux-en-Y gastric bypass surgery that occurred 2 years ago.
Upon physical examination, she is afebrile. Her abdomen is soft and nontender with no masses.
Laboratory studies are shown below in the Table.
| Laboratory study | Value | Normal range |
| WBC count | 7,700/µL | 3,200-9,800/µL |
| Hemoglobin | 13.2 g/dL | 11-14 g/dL |
| Platelets | 215,000/µL | 150,000-450,00/µL |
| Albumin | 4.3 g/dL | 3.5-5.5 g/dL |
| AST | 334 U/L | 5-52 U/L |
| ALT | 282 U/L | 7-46 U/L |
| Alkaline phosphatase | 115 U/L | 40-100 U/L |
| Total bilirubin | 1.7 mg/dL | 0.2-1.5 mg/dL |
| Amylase | 42 U/L | 30-110 U/L |
| Lipase | 24 U/L | 13-141 U/L |
ALT, alanine transaminase; AST aspartate aminotransferase; WBC, white blood cell.
Ultrasonography of the abdomen demonstrates a normal-appearing liver, mild distension of the gallbladder with several stones in the fundus of the gallbladder, and no apparent wall thickening or pericholecystic fluid. The common bile duct is dilated to 1.3 cm.
What is the next most appropriate step in the management of this patient's condition?
This question appears in Med-Challenger Family Medicine Exam Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!
![]()


It's Open Appendectomy Quiz Time with Med-Challenger!
It's Ectopic Pregnancy Quiz Time with Med-Challenger!
It's Cutaneous Disorders Quiz Time with Med-Challenger!