Key takeaway: Adolescent anterior tibial tubercle pain from Osgood–Schlatter is treated with pain control plus *activity modification and flexibility/strengthening*, not routine immobilization or advanced imaging.
Question – Anterior knee pain
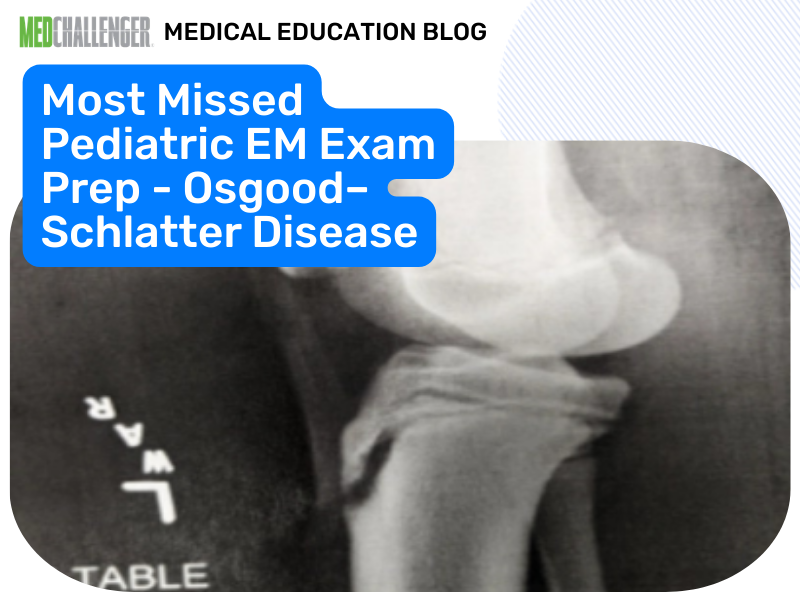
A 12 yo boy presents to the ED with anterior left knee pain. He has been having pain on-and-off for several weeks, beginning when he started playing basketball for his school team. Yesterday, the pain was worse, and he had to sit out of a game, which his father states is unusual for him. He denies any specific injury, and he denies any “pops” or feeling of instability in the knee. He took ibuprofen prior to arrival, and this helped alleviate some of the pain. He has not tried any other treatment modalities. On exam, he has point tenderness on the proximal anterior tibia in the midline of the lower leg. He has no edema of the knee itself, and the knee is grossly stable. He has no pain with internal and external rotation of the hip. He ambulates normally but states it will hurt to run or jump. The following radiograph is obtained.

Image by exclusive permission of personal collection of Ashley Barrile, M.D. All rights reserved
Which of the following is the best treatment strategy?
Answer Options:
- A. NSAIDs and icing for pain control, continuation of activity as long as pain resolves within 24 hours, quadriceps and hamstring stretching exercises
- B. Obtain CT scan of the knee for further assessment of tibial plateau fracture
- C. Place patient in a knee immobilizer and have him follow up with orthopedic surgery as an outpatient
- D. Restrict from activities that cause pain and treat symptoms supportively with NSAIDs and icing
In this item, the keyed answer (A) is directionally aligned with current standard management (conservative care with symptom control and stretching/rehab, with relative activity modification rather than mandatory cessation). However, the explanation’s “24-hour” rule is not a universally stated guideline threshold; major references (e.g., AAOS OrthoInfo and UpToDate updates within the last decade) emphasize pain-guided activity modification and gradual return rather than a strict time-based cutoff.
That said, among the provided options, A remains the best answer because it includes the full conservative package clinicians are expected to recognize for boards: ice/NSAIDs + quadriceps/hamstring stretching (often via PT/HEP) + continued participation as tolerated with modification. Option D is close, but it frames management as “restrict” from painful activities without explicitly incorporating the rehab component that is central to recovery and recurrence prevention.
Why This Pediatric Emergency Medicine Question Is Often Missed
- Test-takers confuse Osgood–Schlatter (benign overuse apophysitis) with acute fracture/avulsion and over-order CT or immobilize.
- Many over-interpret “activity modification” as strict sports prohibition rather than relative rest guided by pain.
- Some miss that rehab (stretching/strengthening) is part of first-line care, not an optional add-on.
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| A. |
Conservative care + activity as tolerated + flexibility rehab |
Best match to guideline-consensus management for Osgood–Schlatter (AAOS/UpToDate). The “24 hours” framing is extra, but the overall strategy is correct. |
| B. |
Concern for occult tibial plateau fracture needing CT |
No acute trauma, no effusion/instability, and exam localizes to tibial tubercle region; CT is not indicated for classic traction apophysitis. |
| C. |
Immobilization and ortho follow-up as if ligament/meniscus/patellar instability |
Routine knee immobilizer is not standard for Osgood–Schlatter; may worsen stiffness/deconditioning and is reserved for certain acute injuries or severe cases under specialist guidance. |
| D. |
Pure activity restriction + symptomatic care |
Too narrow: activity modification is appropriate, but comprehensive management typically includes stretching/strengthening (often PT) to address tight quads/hamstrings and biomechanics. |
High-Yield Pearl for Exam Prep
Osgood–Schlatter = tibial tubercle traction apophysitis treated with ice/NSAIDs + stretching/strengthening and **relative rest/activity modification**, not immobilization or advanced imaging.
Core Learning Objectives
- Differentiate Osgood–Schlatter disease from acute knee trauma requiring immobilization or CT/MRI.
- Select first-line, guideline-consistent management for traction apophysitis in adolescent athletes.
The Exam “Test Trick” at Play
The stem pushes you toward “something structural” (radiograph + point tenderness) and tempts over-management (CT, immobilizer). Boards reward recognizing the classic overuse pattern (weeks of activity-related anterior tibial tubercle pain, stable knee, no acute injury) and choosing conservative, rehab-forward care with pain-guided activity modification.
Additional Peds EM Practice Questions and Remediation for Osgood–Schlatter / Adolescent Overuse Knee Pain
Pediatric Emergency Medicine Practice Question 1 — Classic tibial tubercle pain
A 13-year-old soccer player has 6 weeks of anterior knee pain localized to the tibial tubercle, worse with jumping, improved with rest. Knee is stable; no effusion; X-ray shows fragmented tibial tubercle apophysis. Best initial management?
- A. Long-leg cast for 4 weeks
- B. Ice/NSAIDs + activity modification + quadriceps/hamstring stretching program
- C. CT to exclude tibial plateau fracture
- D. Emergent orthopedic consultation for operative fixation
- E. Complete cessation of all sports until asymptomatic for 6 months
Pediatric Emergency Medicine Practice Question 2 - When to image more
A 12-year-old basketball player has anterior knee pain. Today he felt a “pop” during takeoff and now cannot extend the knee against gravity; there is a large effusion. Next best step?
- A. Reassurance and stretching exercises only
- B. Return to play as tolerated
- C. Immobilize, provide analgesia, and obtain urgent imaging/orthopedic evaluation for extensor mechanism injury
- D. Diagnose Osgood–Schlatter and discharge without precautions
- E. CT for tibial plateau fracture as the first test in all cases
Pediatric Emergency Medicine Practice Question 3 - Activity counseling
A 14-year-old with Osgood–Schlatter asks if he must stop all sports. Best counseling?
- A. Sports are contraindicated until the apophysis fuses
- B. Modify activity to keep pain tolerable; limit aggravating drills and increase as symptoms allow
- C. Continue full activity regardless of pain to avoid deconditioning
- D. Use opioids to allow full participation
- E. Immediate surgical referral for definitive treatment
Pediatric Emergency Medicine Practice Question 4 - Key exam differentiator
Which finding most supports Osgood–Schlatter over patellar tendon rupture?
- A. Sudden onset after a single jump with immediate swelling
- B. Weeks of pain worsened by running/jumping with focal tibial tubercle tenderness and stable knee
- C. Inability to perform straight-leg raise
- D. High-riding patella on exam
- E. Large hemarthrosis
Pediatric Emergency Medicine Practice Question 5 - Management nuance
A 13-year-old with Osgood–Schlatter has persistent pain despite NSAIDs and basic stretching. Next best step?
- A. Immediate CT scan
- B. Formal physical therapy focusing on flexibility/strengthening and biomechanics; consider patellar tendon strap
- C. Knee arthroscopy
- D. Empiric antibiotics
- E. Immediate non-weight-bearing for 8 weeks
Mini Case Discussion Prompt
How would your workup and disposition differ between (1) classic Osgood–Schlatter symptoms over weeks with stable knee and (2) sudden anterior knee pain after a jump with extensor lag and effusion?
Mini-FAQ
- Q1: Do I need CT or MRI to diagnose Osgood–Schlatter?
A: Usually no—ABP/PEM-style exams expect recognition based on history/exam; plain radiographs may be used to rule out other pathology when uncertain, but advanced imaging is uncommon without red flags.
- Q2: Is complete sports cessation required?
A: No—exam standards align with relative rest/activity modification guided by pain plus rehab (AAOS/UpToDate consensus).
- Q3: When is immobilization appropriate?
A: Not for uncomplicated Osgood–Schlatter; immobilization is reserved for suspected acute structural injury (e.g., extensor mechanism injury) or select severe cases under specialist direction.
- Q4: What’s the key rehab emphasis for board questions?
A: Stretching/strengthening (especially quadriceps/hamstrings, and overall biomechanics) plus gradual return to activity—this is what differentiates optimal care from “just NSAIDs.”
Find this and other Pediatric Emergency Medicine exam prep questions in Med-Challenger Pediatric Emergency Medicine 3rd Edition Exam Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements.