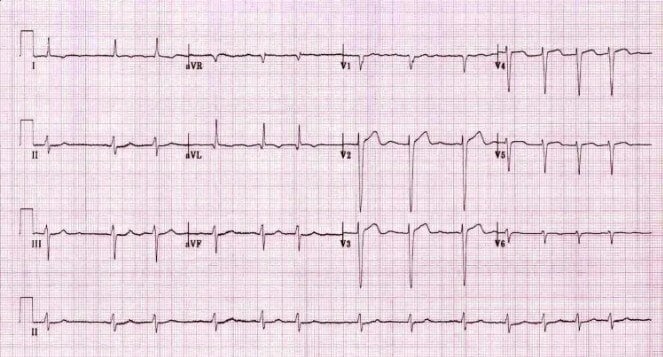
A 67-year-old woman with a history of chronic congestive heart failure caused by cardiomyopathy has the ECG tracing shown below. What can be stated about the ECG?
Answers:
- Right bundle branch block with 2 positive Sgarbossa criteria
- Left anterior fascicular block
- Left bundle branch block, negative Sgarbossa criteria
- Possible acute myocardial infarction
The correct answer is 4, possible acute MI.
The incorrect answer chosen most often is 2, left anterior fascicular block.
There's not really an exam trick to this question, it's meant to (1) determine whether you distinguish LBBB in the ECG, and then (2) see if you apply Sgarbossa criteria. There's nothing tricky, it is a standard depth-of-knowledge question. Of course, it is kind of a critical depth of knowledge issue...
Why This Question Is Often Missed
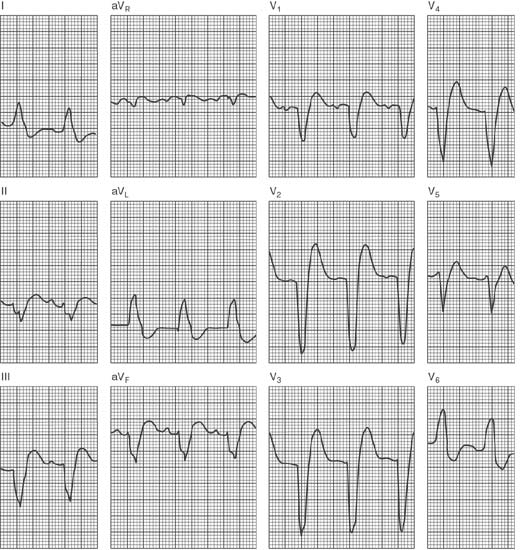
- Clinicians often misidentify the wide, notched QRS complexes as RBBB or fascicular blocks instead of classic LBBB patterns (broad R in I/aVL; deep S in V₁–V₂).
- ST‑segment changes in LBBB are too easily dismissed as “secondary repolarization,” so Sgarbossa criteria for acute MI are overlooked.
Which matches the learning objectives designed into the question:
- Distinguish LBBB by QRS ≥ 120 ms with broad/notched R in I, aVL, V₅–V₆ and deep S in V₁–V₂.
- Apply Sgarbossa criteria (original and modified) to detect acute MI in the presence of LBBB.
High‑Yield Pearl
In presumed-new LBBB, ≥1 mm concordant ST‑elevation or depression in any lead is nearly 100% specific for acute MI (Sgarbossa).
What the Distractors Indicate
| Option | What It Tests / Implies | Why It’s Wrong Here |
|---|---|---|
| Right bundle branch block with 2 positive Sgarbossa criteria |
Recognition of RBBB morphology and use of Sgarbossa in RBBB | QRS‑axis and morphology lack rSR′ in V₁ and wide S waves laterally—this is LBBB, not RBBB, so Sgarbossa can’t apply. |
| Left anterior fascicular block | Identification of axis deviation without full BBB | Although the axis may be leftward, QRS duration (>120 ms) and broad notched patterns confirm LBBB, not LAFB alone. |
| Left bundle branch block, negative Sgarbossa criteria |
Correct block identification but assumes no MI evidence | Here, there are concordant ST‑segment deviations meeting Sgarbossa thresholds—criteria are positive for MI. |
| Possible acute myocardial infarction |
Application of Sgarbossa criteria to diagnose MI in LBBB | Correct: Concordant ST changes in LBBB fulfill Sgarbossa criteria for acute MI. |
Additional Test Questions Related to Learning Objectives
Question 1
A 68‑year‑old man with dyspnea has an ECG showing QRS 140 ms, a broad monophasic R in lead I, and a deep S in V₁. Which conduction abnormality is present?
-
A. Right bundle branch block
-
B. Left anterior fascicular block
-
C. Left bundle branch block
-
D. Nonspecific intraventricular conduction delay
Question 2
A 72‑year‑old woman with known LBBB and 90 min of chest pain has 2 mm ST‑elevation in lead V₂, concordant with the QRS. What does this most likely represent?
-
A. Secondary ST‑T changes of chronic LBBB
-
B. Acute myocardial infarction
-
C. Early repolarization
-
D. Digoxin effect
Question 3
A 75‑year‑old man with new LBBB has 5 mm ST‑depression in lead V₆ and a 20 mm R wave amplitude there. Using the modified Sgarbossa ratio (ST‑depression/QRS ≤ –0.25), does this meet criteria for acute MI?
-
A. Yes, ratio = –0.25
-
B. No, ratio is too small
-
C. Cannot apply in LBBB
-
D. Suggests pericarditis
Group Discussion Prompt
Discuss how the modified Sgarbossa (Smith) criterion enhances sensitivity over the original rule in LBBB-associated MI diagnosis, and identify any remaining diagnostic limitations.