Many learners miss this week’s top family-medicine question on Eisenmenger risk because they focus on shunt size rather than shunt pressure. This breakdown explains why a PDA progresses faster than other congenital lesions and how to recognize the physiologic trap on exams.
Which of the following congenital heart lesions, if left untreated, is most likely to lead to Eisenmenger syndrome?
Answer Options:
- atrial septal defect
- patent ductus arteriosus
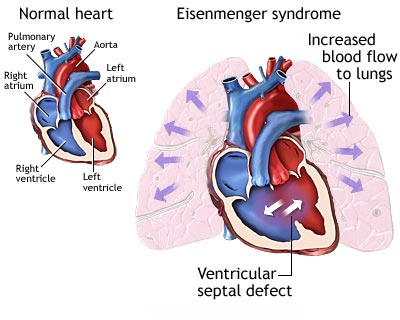
- ventricular septal defect
- bicuspid aortic valve with or without aortic stenosis
The correct answer is #2. This week’s most-missed family-medicine question asks which congenital lesion most often leads to Eisenmenger. The key lies in understanding pressure-driven shunting—especially the unique hemodynamics of a PDA.
Why This Question Is Often Missed
-
Confusing Shunt Magnitude vs. Pressure Gradient
Students often know that VSDs create large shunts but overlook that a PDA’s anatomy directs high‐pressure aortic flow straight into the pulmonary circulation, accelerating vascular remodeling.
-
Assuming All Left‑to‑Right Lesions Behave Alike
It’s tempting to lump ASD, VSD, and PDA together; however, differences in pressure gradients and shunt pathways change the timeline for developing Eisenmenger physiology.
What the Distractors Indicate
| Option |
What It Tests / Implies |
Why It’s Wrong Here |
| Atrial septal defect |
Recognition of a low‑pressure left‑to‑right shunt |
The shunt gradient is lower and reversal takes decades—Eisenmenger is very uncommon early. |
| Ventricular septal defect |
Awareness of high‑volume septal defects |
Although VSDs can cause Eisenmenger, the direct aorta‑to‑pulmonary flow in PDA accelerates it sooner. |
| Bicuspid aortic valve (± stenosis) |
Identification of obstructive or valvular lesions, not shunts |
No left‑to‑right shunt exists—does not increase pulmonary blood flow or pressure. |
High-Yield Pearl
A PDA exposes the pulmonary vasculature to systemic pressures and flow continuously, making it the lesion most prone to early pulmonary vascular remodeling and Eisenmenger reversal.
Core Learning Objectives
- Recognize which congenital heart defects create sustained high‑pressure, high‑volume left‑to‑right shunts that predispose to pulmonary vascular remodeling.
- Distinguish lesions by their anatomic shunt pathway and pressure gradient to predict the timeline for progression to Eisenmenger syndrome.
The “Test Trick” at Play
This question leverages the tactic of emphasizing “most likely” rather than simply “can lead to.” It tests your ability to compare both shunt magnitude and the directness of flow from systemic to pulmonary circuits. PDA uniquely channels aortic pressure into the pulmonary artery without an intervening chamber, so it drives pulmonary hypertension faster than septal defects.
Additional Family Medicine Practice Questions and Remediation
FM Exam Prep Practice Question 1
A 6‑year‑old child presents with a continuous, “machine‑like” murmur best heard at the left infraclavicular area and bounding peripheral pulses. There are early signs of pulmonary hypertension on echo. Which lesion most likely explains these findings?
A. Patent ductus arteriosus
B. Atrial septal defect
C. Ventricular septal defect
D. Bicuspid aortic valve
FM Exam Prep Practice Question 2
A teenager with a history of a mild murmur in infancy now presents with clubbing of fingers, exercise intolerance, and right ventricular hypertrophy on ECG. He never received surgical repair. Which congenital lesion most likely progressed to Eisenmenger physiology in this patient?
A. Large ventricular septal defect
B. Patent ductus arteriosus
C. Secundum atrial septal defect
D. Pulmonic stenosis
FM Exam Prep Practice Question 3
An adult patient presents with late‑onset cyanosis, clubbing, and a history of a “split S2” murmur as a child. Echo shows right‑to‑left shunting at the atrial level and marked pulmonary arterial hypertension. Which defect most likely led to this picture?
A. Ostium secundum atrial septal defect
B. Patent ductus arteriosus
C. Coarctation of the aorta
D. Bicuspid aortic valve
Mini Case Discussion Prompt
How would you tailor the timing and type of intervention (e.g., device closure vs. surgical ligation) for different left‑to‑right shunts—such as PDA, VSD, and ASD—to prevent progression to pulmonary vascular disease, and what patient‑ or lesion‑specific factors influence this decision?
This question appears in Med-Challenger Family Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!

No matter your program, no matter the size, Med-Challenger for Groups and Institutions can better prepare your program or group, fulfill industry requirements, and increase test scores.
For personal medical education that includes board's prep, MOC, and CME requirements, Med-Challenger has you covered in Family Medicine, Emergency Medicine, Internal Medicine, Pediatrics, Pediatric Emergency Medicine, OBGYN, Physician Assistants, and Nurse Practitioners.
Never miss a thing. Subscribe to our blog and save!