Mycoplasma pneumoniae
A large number of microorganisms cause pneumonia, ranging from viruses to bacteria and fungi. The etiologic agents of pneumonia depend on the patient’s age. In neonates (0-3 months of age), maternal flora, such as group B streptococcus and gram-negative bacteria, are common vertically transmitted causes. In children older than 1 week, viruses account for 14% to 35% of cases; in this group, Streptococcus pneumoniae remains the most common bacterial cause of pneumonia. However, in certain age subcategories, the pattern of infections deviates from the overall statistics. For example, in children aged 3 months to 5 years, 50% to 60% of all cases of pneumonia are viral. By contrast, in school-aged children (aged > 5 years), atypical organisms, such as M pneumoniae and Chlamydophila pneumonia (previously known as C pneumoniae), are more common. M pneumonia, classified as an atypical pneumonia, remains the leading cause of pneumonia in school-age children and young adults.
It is difficult to clinically differentiate bacterial from viral pneumonia. Bacterial pneumonia might have a more abrupt and severe onset after days of symptoms of upper respiratory tract infection. Bacterial pneumonia is also more likely to result in clinical complications. Wheezing in a child older than 5 years with signs of pneumonia will typically be due to atypical bacterial and viral pneumonias and is unlikely to be due to other bacterial causes.
M pneumoniae infection may be asymptomatic or may present with minimal physical examination findings. If the symptoms are compatible with atypical bacterial pneumonia and are clinically significant, then coverage using a macrolide (azithromycin or clarithromycin) should be considered.
A less common source for an atypical bacterial pneumonia is C pneumonia, which usually presents with abrupt onset of fever, malaise, myalgia, headache, photophobia, sore throat, and gradually worsening and prolonged, nonproductive cough. Hoarseness is more frequently seen with C pneumoniae infection compared with pneumonia of a viral origin.
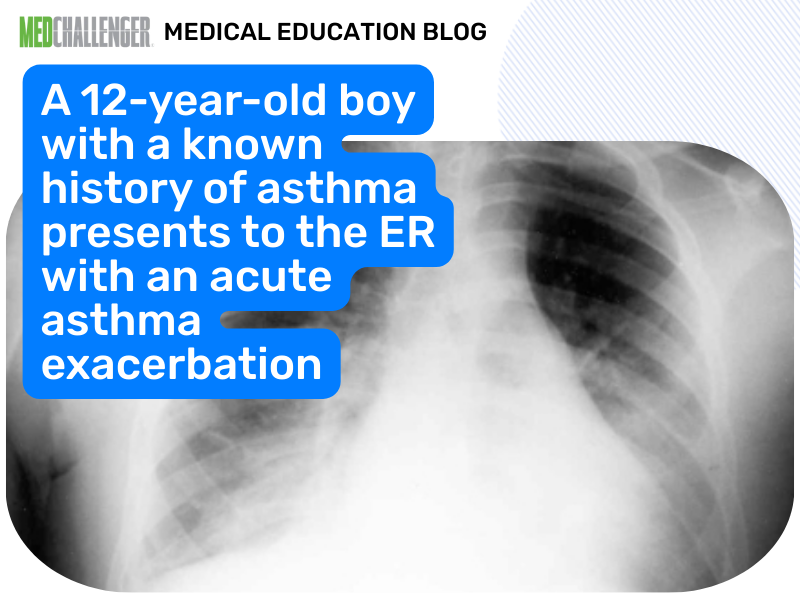
Pneumonia is defined as lower respiratory tract infection typically associated with fever, respiratory symptoms, and evidence of parenchymal involvement by either physical examination or the presence of infiltrates on chest radiography. It is due to an inflammatory process of the lungs that may affect the airways, alveoli, connective tissue, visceral pleura, and vascular structures.
Radiologically, pneumonia is defined as an infiltrate on an chest x-ray in a child with symptoms of an acute respiratory illness.
References:
Gereige RS, Laufer PM. Pneumonia. Pediatr Rev. 2013;34(10):438-456.
Hanhan U, Orlowski J, Fiallos M. Association of Mycoplasma pneumoniae infections with status asthmaticus. Open Respir Med J. 2008;2:35-38.
.png?width=433&height=301&name=image%20(60).png)
/PEDS%20CHALLENGER.png?width=250&height=218&name=PEDS%20CHALLENGER.png)

