Product News
November 20, 2025 Newsletter
ABOG certifying exam tips and this week's most‑missed OB/GYN questions—quick exam‑prep insights and practice links from Challenger.
Most missed EM exam question: recognizing NAVA (neurally adjusted ventilatory assist) vs time/pressure modes. Quick tips and practice for exam prep.
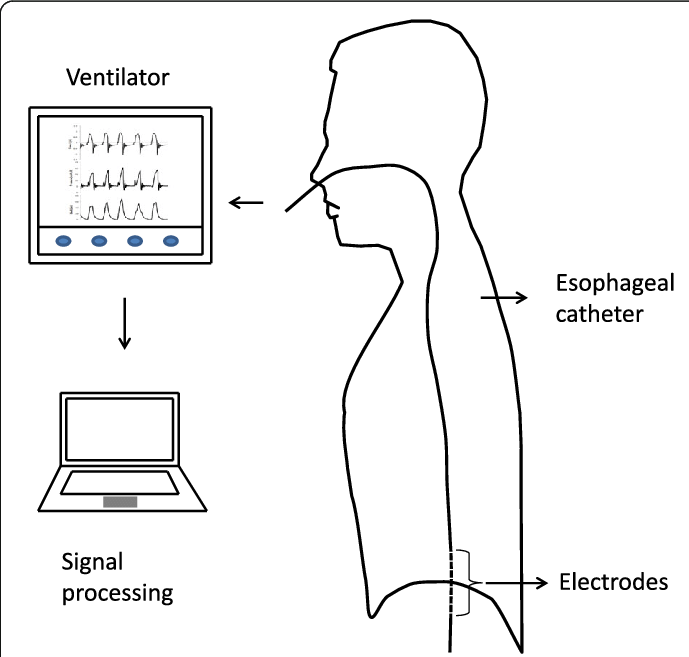
The most‑missed concept is recognizing NAVA (neurally adjusted ventilatory assist) — a neurally triggered ventilator mode using diaphragmatic EMG to time and proportion assistance, unlike time‑ or pressure‑triggered modes.
You intubate a 9-year-old with refractory asthma. Which mode of ventilation will reduce dyssynchrony with its attendant risk of ventilator-induced lung injury?

Answer Options:
The correct answer is (1) - NAVA.
While not a tricky question, 'no PEEP' is more a strategy than a ventilation mode, so it could perhaps be worded better. But the focus of the question is on the familiarity with American Thoracic Society's pediatric ventilator management guideline. (Or the European Society of Paediatric and Neonatal Intensive Care - ESPNIC.)
#4, 'no PEEP', is the most common incorrect answer to this question.
– Unfamiliarity with NAVA: Many learners haven’t encountered Neurally Adjusted Ventilatory Assist in routine training, so they default to more common modes (SIMV, AC).
– Misleading “No PEEP” option: Trainees may think removing PEEP reduces auto‑PEEP and thus dyssynchrony, but eliminating PEEP can worsen dynamic hyperinflation and asynchrony.
| Option | What It Tests / Implies | Why It’s Wrong Here |
|---|---|---|
| Synchronized Intermittent Mandatory Ventilation (SIMV) |
Understanding of mandatory vs spontaneous breath timing | SIMV still delivers mandatory breaths at set times and can lead to asynchrony when patient effort doesn’t match set breaths. |
| Assist Control Ventilation (AC) |
Knowledge of full support volume/pressure control | AC delivers every breath fully supported regardless of patient effort, risking overassist and dyssynchrony. |
| No Positive End‑Expiratory Pressure (PEEP) |
Concept that PEEP removal may lower auto‑PEEP and improve synchrony | Removing PEEP increases collapse and dynamic hyperinflation, worsening synchrony and VILI risk. |
NAVA utilizes diaphragmatic EMG signals to trigger and cycle breaths in synchrony with patient effort.
This question pushes you to recognize a cutting‑edge mode rather than defaulting to familiar settings; it tests whether you can distinguish a mode driven by neural signals (NAVA) from time‑ or pressure‑triggered modes, a nuance often overlooked under exam pressure.
A 10‑year‑old with status asthmaticus remains dyssynchronous on AC ventilation despite deep sedation. Which mode best restores synchrony and minimizes VILI risk?
Which ventilator mode senses the electrical activity of the diaphragm to synchronize assistance with patient effort?
A 7‑year‑old intubated for severe bronchiolitis exhibits marked patient–ventilator dyssynchrony. Beyond optimizing sedation, which adjustment directly targets neural synchrony?
Discuss how you would integrate sedation strategies when initiating NAVA in a pediatric asthma patient, and compare the advantages and limitations of neurally adjusted ventilatory assist versus pressure support ventilation in this context.
This question appears in Med-Challenger Emergency Medicine Review with CME
Try for free and save. Ace your exams and meet your CME/MOC requirements for just $35 a month!



ABOG certifying exam tips and this week's most‑missed OB/GYN questions—quick exam‑prep insights and practice links from Challenger.
Most-missed Pediatric Emergency Medicine question on necrotizing fasciitis — quick answer, key exam clues, and high-yield pearl for Peds EM exam prep.
Most Missed Question in Pediatric Emergency Medicine: concise answer, why it's missed, and a testing tip for PEM exam prep.