Sodium bicarbonate
Educational Objective:
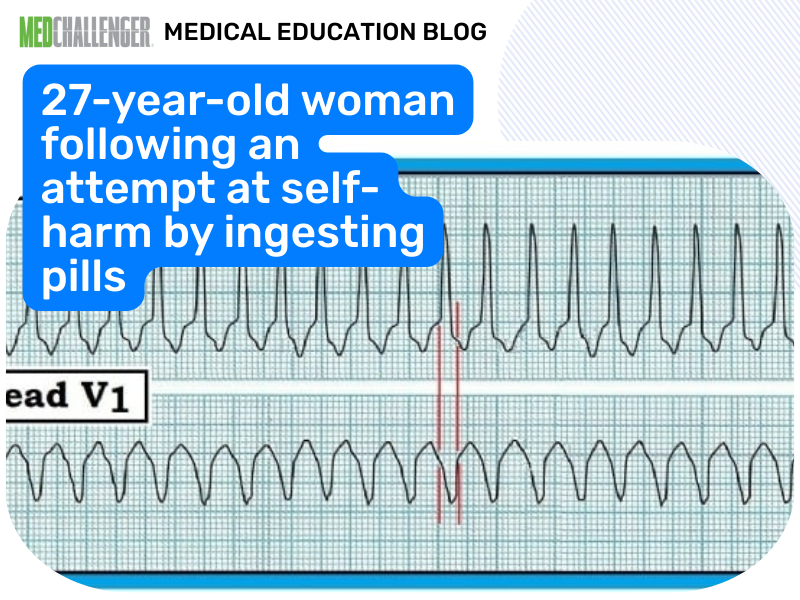
Identify toxic exposures in which bicarbonate is an appropriate initial therapy.
Key Point:
The electrocardiogram demonstrates a widened QRS interval (over 100 ms or over 2.5 small ECG boxes), which is indicative of the patient having ingested an antimuscarinic agent with concomitant sodium channel blockade (e.g. large dose of diphenhydramine or ingestion of tricyclic antidepressant with antimuscarinic and sodium channel blocking side effects).
Explanation:
The QRS widening in this context is potentially life-threatening because it predisposes the patient to fatal ventricular arrhythmias and seizures. Sodium bicarbonate is the appropriate therapy for this situation.
Physostigmine, which may normally be indicated as an antidote in an antimuscarinic overdose, is initially contraindicated in this situation because the antimuscarinic toxidrome itself is not immediately life-threatening and physostigmine will only treat the antimuscarinic toxidrome, not the concomitant life-threatening sodium channel blockade.
Urinalysis to screen for drugs of abuse would not significantly add to the management of this patient’s condition and would delay the administration of appropriate therapy. Similarly, a serum electrolyte panel would delay potentially life-saving sodium bicarbonate treatment in this patient.
Review:
Physostigmine is a tertiary carbamate that, like organophosphorus-containing compounds, inhibits acetylcholinesterase and thereby increases the amount of acetylcholine present in the synaptic cleft. This larger amount of acetylcholine in the synaptic cleft outcompetes the toxic toxic compound for muscarinic acetylcholine receptors.
Reference:
Monte AA. Anticholinergics. (Chapter 145) In: Walls R, et al. Rosen’s Emergency Medicine: Concepts and Clinical Practice. 9th ed., 2018: 1863-1867.e2